


The US Leader in Stem Cell Therapy, Now in Mexico. Treatments start at $3,999 for 25 million stem cells!
Special Promo: Get an additional 25 BILLION Exosomes IV with treatments over 50 million cells!
Pricing Notice: Prices updated June 1, 2026; please see this page for current rates as past ads/videos may be outdated.
The US Leader in Stem Cell Therapy, Now in Mexico. Treatments start at $3,999 for 25 million stem cells!
Special Promo: Get an additional 25 BILLION Exosomes IV with treatments over 50 million cells!
Pricing Notice: Prices updated June 1, 2026; please see this page for current rates as past ads/videos may be outdated.
Written by Dr. David Greene, MD, PhD, MBA on July 16, 2026
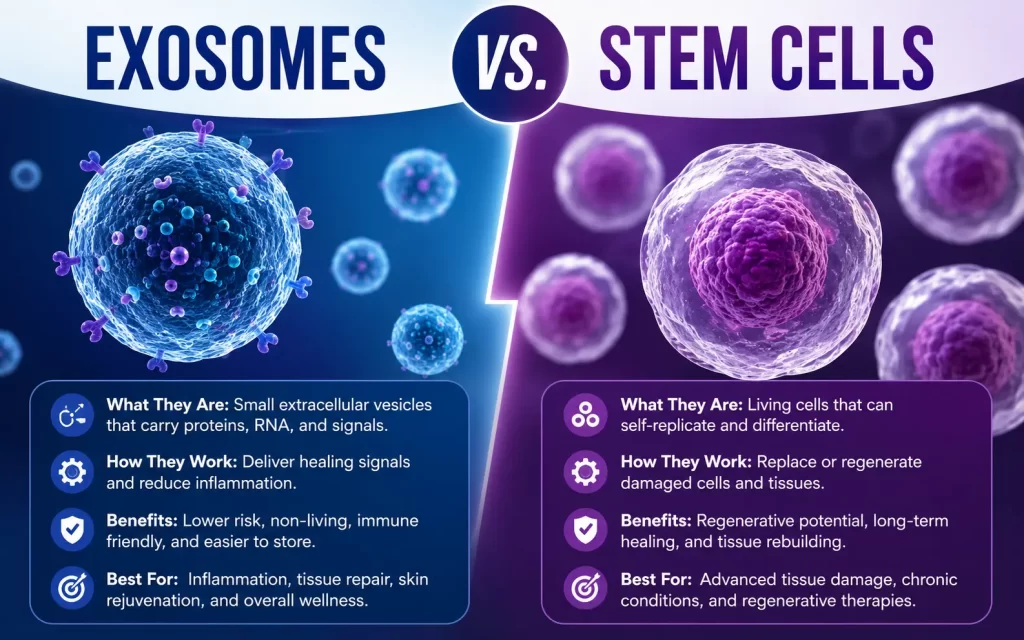
Stem cells are living cells that can divide, replicate, and transform into other specialized cell types (like cartilage, bone, or nerve cells). Exosomes are not cells at all, they're microscopic, membrane-bound vesicles that cells release to carry messenger molecules (growth factors, proteins, and RNA) to other cells. In short: stem cells become new tissue; exosomes deliver instructions that help existing cells repair themselves.
If you’ve been looking into new medical treatments… you’ve probably heard about stem cells and exosomes. Both are creating BIG waves in the medical world. But here’s the thing, they’re NOT the same. Not even close.
Let me break this down for you.
| Feature | Stem Cells | Exosomes |
|---|---|---|
| What it is | A living cell | A cell-derived vesicle (not a cell) |
| Size | ~15–20 microns (about 100× larger than an exosome) | 30–150 nanometers |
| Has a nucleus | Yes | No |
| Can replicate (divide) | Yes | No |
| Can differentiate into other cell types | Yes | No |
| Typical dose per treatment | Tens of millions of cells | Billions of vesicles |
| Primary role | Regenerate or replace damaged tissue | Cell-to-cell signaling and repair instructions |
| FDA approval status (U.S., as of 2026) | Approved only for specific hematopoietic (blood/immune) indications; most other uses remain investigational. | No FDA-approved exosome therapeutic products; research and IND-cleared clinical trials only. |
A stem cell is a living, biological cell — complete with a nucleus and its own DNA. What makes it unique among cells is two abilities:
Stem cells are sourced from bone marrow, adipose (fat) tissue, umbilical cord tissue, and — in research settings — embryos and induced pluripotent stem cells (adult cells reprogrammed to an earlier, more flexible state).
Regulatory status: In the United States, the FDA has approved a small number of stem cell-based products, primarily hematopoietic (blood-forming) stem cell transplants for blood cancers and immune disorders, along with several umbilical cord blood-derived products for specific hematologic conditions. In December 2024, the FDA approved the first mesenchymal stromal cell (MSC) therapy, remestemcel-L, for a form of pediatric graft-versus-host disease. Outside of these specific, FDA-cleared indications, most other stem cell applications — including many used for orthopedic and degenerative conditions — remain investigational in the U.S. and are not FDA-approved.
Known limitations: Because stem cells are relatively large physical particles, intravenous infusion can cause some cells to become trapped in the lungs (“first-pass entrapment”). The immune system may also recognize donor cells as foreign, and — though rare — abnormal cell growth is a theoretical risk with any therapy involving living, replicating cells. These are among the reasons stem cell products face a more rigorous, cell-by-cell regulatory pathway.
Exosomes are not cells — they’re tiny, fat-encased vesicles that cells naturally release as a form of communication. Picture a soap bubble: a cell packages growth factors, proteins, lipids, and messenger RNA inside a lipid membrane, then releases that bubble into the bloodstream or surrounding tissue.
Once released, exosomes travel to nearby or distant cells, are absorbed, and release their molecular cargo — effectively delivering repair signals without becoming part of the recipient tissue themselves. Every cell type produces exosomes, and they’re found throughout the body in blood, saliva, urine, breast milk, and other fluids. In regenerative medicine, the exosomes of clinical interest are typically derived from mesenchymal stem cells, since they appear to carry a concentrated set of the same regenerative signaling molecules the parent stem cells use to support tissue repair.
Regulatory status: As of 2026, there are no FDA-approved exosome therapeutic products in the United States. Several exosome-based candidates are in Phase I/II clinical trials under FDA Investigational New Drug (IND) clearance for conditions ranging from wound healing to neurological and cardiovascular disease, but exosome therapy — including for orthopedic and aesthetic uses — remains investigational. The FDA has issued public safety communications warning about unapproved stem cell and exosome products marketed without adequate clinical evidence.
The scale difference between the two is enormous. An exosome measures 30–150 nanometers — roughly 1/100th the size of a single stem cell. Because they’re so much smaller, a single treatment vial can contain billions of exosomes compared to tens of millions of stem cells. This is a normal, expected difference in how each product is measured — not an indication that one is “more concentrated” or superior to the other.
A note on marketing claims: If a provider advertises “billions of stem cells” in a single treatment, that claim doesn’t reflect how stem cell products are typically dosed or measured — a realistic stem cell dose is in the tens of millions of cells, not billions. Large-vial-count claims usually refer to exosomes, not stem cells. It’s reasonable to ask any provider exactly what cell type and quantity you’re receiving, and to ask for that information in writing.
Stem cells work primarily in two ways: by migrating to damaged tissue and potentially differentiating into replacement cells, or by secreting their own signaling molecules (including exosomes) that recruit the body’s own repair processes.
Exosomes work exclusively through signaling. They circulate until they encounter a damaged or inflamed cell, are taken up by that cell, and release growth factors and genetic instructions that can influence inflammation, tissue repair, and cell survival — without the exosome itself becoming new tissue.
Research is ongoing into applications for both approaches across orthopedic, autoimmune, neurological, and wound-healing conditions. Evidence quality varies significantly by condition and application, and much of this research remains preclinical or early-phase.
More than 1,100 mesenchymal stem cell (MSC) clinical trials had been registered worldwide as of 2023, though only a small number of MSC-derived products have received full regulatory approval globally — most of those approvals are in South Korea, Japan, and other parts of Asia rather than the U.S.
Approximately 240 exosome-related clinical trials were registered globally between 2011 and early 2024, spanning oncology, cardiovascular disease, neurological disorders, and wound healing. Roughly a fifth of these are interventional (testing an actual treatment) rather than diagnostic.
Global market analysts project continued growth in both fields over the next several years, though market size projections vary widely between reports and should be read as estimates, not guarantees of clinical availability or approval.
Because manufacturing standards, dosing, and purity can vary significantly between exosome products and producers, the FDA and researchers alike have emphasized the need for standardized manufacturing and quality control as the field matures.
Some regenerative medicine providers use both together, reasoning that stem cells provide potential tissue-building capacity while exosomes support the surrounding inflammatory and signaling environment. Whether a combination, single-cell, or exosome-only approach is appropriate depends on the individual’s condition, and should be discussed with a qualified medical provider — this article does not constitute a treatment recommendation.
No. An exosome is not a cell at all — it has no nucleus and cannot divide or turn into other cell types. Exosomes are vesicles that cells (including stem cells) release to carry signaling molecules to other cells.
No. As of 2026, there are no FDA-approved exosome therapeutic products in the United States. Exosome-based treatments are available only through registered clinical trials or as unapproved products, and the FDA has issued public warnings about unregulated exosome and stem cell products.
Both have different risk profiles. Because exosomes are not living cells, they carry a lower theoretical risk of abnormal growth or graft-versus-host complications compared with donor stem cells, but they are less studied overall and manufacturing standardization is still developing. Ask any provider for details on sourcing, testing, and manufacturing practices before pursuing either therapy.
Because exosomes are roughly 100 times smaller than stem cells, a typical vial can contain billions of exosomes compared with tens of millions of stem cells. This reflects normal differences in scale between the two products, not a difference in potency or quality.
Not necessarily — they serve different biological functions. Exosomes may be studied as a signaling-based alternative for certain applications, but they cannot physically replace or regenerate tissue the way a living stem cell theoretically can. Ongoing clinical trials are evaluating where each approach — or a combination — may be most effective.
This article is for informational purposes only and is not a substitute for professional medical consultation, diagnosis, or treatment. Stem cell and exosome therapies are considered experimental in most applications and are not FDA-approved for the treatment or cure of any condition outside their specific approved indications.
Contact US

Dr. David Greene
MD, PhD, MBA
Dr. David Greene, MD, PhD, MBA, is a pioneering leader in regenerative medicine and healthcare marketing. As a residency and fellowship-trained orthopedic surgeon, Dr. Greene transitioned from clinical practice to become the founder and CEO of R3 Stem Cell and US Lead Network, where he has revolutionized patient care and medical practice growth through innovative therapies and digital marketing strategies. He has authored two influential books on healthcare internet marketing, ranks among the top expert authors globally, and has been featured on the cover of Corporate Vision magazine for his impact on global regenerative therapies. Beyond his professional achievements, Dr. Greene is passionate about education, compassion, and continuous innovation.