


The US Leader in Stem Cell Therapy, Now in Mexico. Treatments start at $3,999 for 25 million stem cells!
Special Promo: Get an additional 25 BILLION Exosomes IV with treatments over 50 million cells!
Pricing Notice: Prices updated June 1, 2026; please see this page for current rates as past ads/videos may be outdated.
The US Leader in Stem Cell Therapy, Now in Mexico. Treatments start at $3,999 for 25 million stem cells!
Special Promo: Get an additional 25 BILLION Exosomes IV with treatments over 50 million cells!
Pricing Notice: Prices updated June 1, 2026; please see this page for current rates as past ads/videos may be outdated.
Written by Dr. David Greene, MD, PhD, MBA on November 27, 2025
Stem cell therapy for macular degeneration is a new kind of treatment that tries to protect or replace damaged cells in the macula so central vision can last longer and, in some cases, even improve a little. Right now, it is still an experimental therapy tested in clinical trials, but early results show that stem cells can help some patients with advanced age‑related macular degeneration (AMD) gain letters on the eye chart and slow further degeneration.
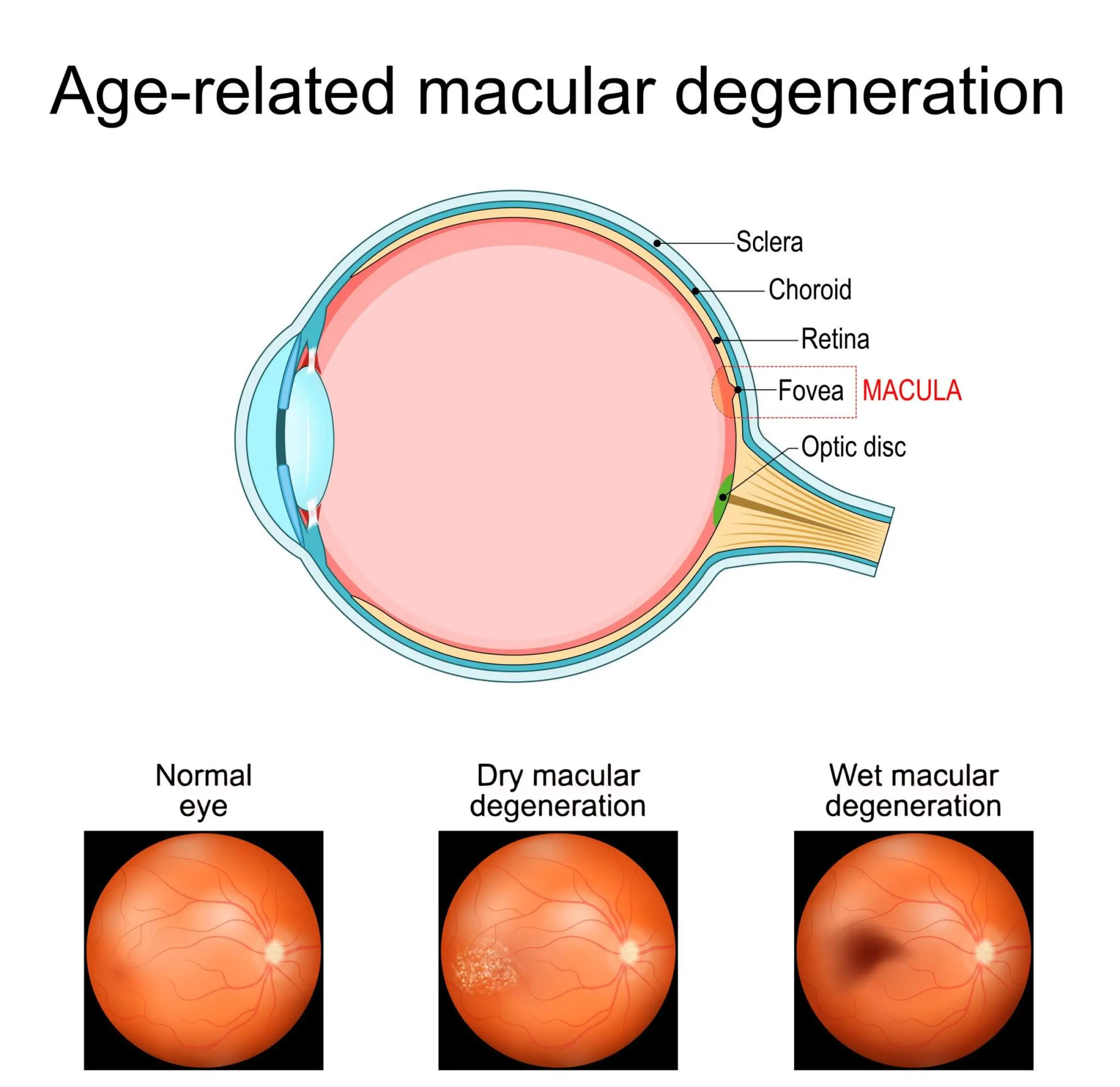
Age‑related macular degeneration is a degenerative disease that affects the macula, the small area in the center of the retina that gives sharp, central vision for reading, driving, and face recognition. Global research shows that AMD affected about 196 million people in 2020 and may reach around 288 million by 2040, indicating that central vision loss will be a significant burden for patients, families, and health systems in the coming decades.
Most people who sit in the exam chair have dry age‑related macular degeneration, which accounts for roughly 80% of AMD cases, while the wet form causes many of the sudden, severe vision drops. Standard treatment for wet AMD uses repeated anti‑VEGF injections into the eye, often every 4–6 weeks, but these injections slow fluid and bleeding; they do not repair dead retinal pigment epithelium (RPE) or lost photoreceptor cells, and there is still no approved therapy that truly reverses dry AMD once geographic atrophy forms.
Here is the basic idea in simple words…. stem cells regenerate retinal tissue. In dry AMD, parts of the RPE layer under the macula die, the pigment epithelium can no longer support the overlying photoreceptors, and central vision fades; stem cell therapy tries to restore or replace those support cells, protect surviving photoreceptors, and slow the path toward blindness.
Different stem cell types play different roles:
Stem cell type
Source
Main retinal goal |
Typical procedure type |
Trial stage |
Embryonic stem cells (ESCs)
Early‑stage embryo cell lines
Make RPE or photoreceptor cells to transplant under the macula
Subretinal cell sheet or cell suspension transplantation
Phase I/II safety and early outcomes
Induced pluripotent stem cells (iPSCs)
Adult cells reprogrammed in the lab
Create patient‑specific retinal cells with less rejection risk
Subretinal transplantation or RPE patch
Early human and preclinical work
Mesenchymal Stem Cells (MSCs)
Bone marrow, fat, or other adult tissue
Support and protect retinal cells by growth factors, not direct replacement
Intravitreal or intravenous injection
Small human series with modest gains
Adult RPE stem cells |
Cells from donor RPE tissue
Replace damaged RPE in advanced dry AMD
Subretinal injection as RPE progenitor suspension
Phase 1/2a trial data now published
In most macula stem cell transplant procedures, a retinal surgeon makes a tiny opening, places a very fine cannula under the retina, and injects a small dose of cells right under the zone of degeneration, then monitors healing and graft position over many months.
The therapy does not feel like magic in the chair; it feels like a precise, advanced eye surgery that must balance regeneration, safety, and long‑term outcomes in very delicate ocular tissue.
Early clinical trials focus first on safety. In a phase 1/2a trial of adult RPE stem‑cell–derived RPE progenitor cells (RPESC‑RPE‑4W) for advanced dry AMD, six patients received a low dose of 50,000 cells under the retina in the worst‑seeing eye; after about 12 months, the three sickest eyes gained an average of a little over 20 ETDRS letters, while the better eyes gained a few letters at six months, and doctors did not see serious product‑related events, tumors, or strong inflammation.
Long‑term follow‑up of a different RPE implant for advanced dry AMD showed that the implant stayed in place, remained safe, and kept a stable structure on scans over a median of three years, which suggests that RPE replacement can work as a long‑term graft in the macula.
For wet AMD, one project in the UK placed a one‑cell‑thick patch of embryonic stem cell‑derived RPE on a synthetic scaffold under the macula in patients with severe neovascular disease that did not respond well to standard care; in early results, one patient gained about 29 ETDRS letters and another gained about 21 letters after roughly a year, while the engineered layer stayed attached and was well tolerated.
Mesenchymal Stem Cell trials—for example, intravitreal autologous bone‑marrow MSC injections in small AMD and inherited retinal disease series—have shown that some patients gain one line or more of vision and show changes in electroretinogram signals, but structural imaging often changes very little, which means functional improvement can appear before the retina “looks” better on scans.
Now comes the part that really matters for anyone reading this with AMD….. safety and trust. Regulated clinical trials report that subretinal RPE cell therapy so far shows an acceptable safety profile in small groups, with no clear signal of tumors and with manageable issues like local inflammation or transient fluid, but the number of patients is still low and follow‑up is still short compared with a lifetime disease.
The bigger danger comes from unregulated clinics that inject “stem cells” from fat or blood directly into the eye without proper cell preparation, dose control, or regulatory review; reports describe at least three women with AMD in the United States who paid thousands of dollars for intravitreal injections and were left with severe, permanent vision loss in both eyes due to complications such as retinal detachment and bleeding. Patient‑education studies show that many people do not realize that, as of now, stem cell therapy for AMD is still classed as experimental and should only take place inside approved, monitored clinical trials run by retinal surgeons and clinical trial coordinators who follow strict safety rules.
Here is a simple checklist to use before any stem cell offer for the macula:
Ask for the clinical trial ID (for example, an NCT number) and look it up on a public registry.
Confirm that an ophthalmologist or retinal surgeon is in charge of the procedure and follow‑up.
Ask clear questions about procedure type (subretinal injection, RPE patch, intravitreal injection), stem cell source (ESCs, iPSCs, MSCs, RPE stem cells), and how safety is monitored over time.
Be careful if a clinic asks for large cash payments, suggests fast vision cures, or tells you not to inform your usual eye doctor.
For some patients, it can also make sense to speak with centers that focus on regenerative eye care and cross‑border treatment, such as R3 Stem Cell Mexico, but any step toward stem cell therapy should still rest on clear clinical evidence, honest talk about risks, and a shared plan with a trusted retina specialist.
Right now, stem cell therapy for age‑related macular degeneration is best seen as an emerging, vision‑saving option that slows degeneration and can sometimes restore part of lost function, but only for selected patients and only under strict study rules.
Clinical trials continue to test different doses, different stem cell sources, and different surgical tools so doctors can better assess effectiveness, long‑term outcomes, and which patients are most likely to experience improved vision rather than risk extra damage.
For anyone living with AMD today, the most practical steps are simple: protect the retina with standard care, follow a regular monitoring plan, ask about clinical trial options in your region, and stay informed about new data as they are published year by year.
Stem cells will not cure every macula, but as research from ophthalmologists, researchers, biotech companies, and regulatory agencies grows, this therapy may move from small experimental studies to safer, more widely available treatments that help many more people keep the gift of central vision for longer.
Contact US

Dr. David Greene
MD, PhD, MBA
Dr. David Greene, MD, PhD, MBA, is a pioneering leader in regenerative medicine and healthcare marketing. As a residency and fellowship-trained orthopedic surgeon, Dr. Greene transitioned from clinical practice to become the founder and CEO of R3 Stem Cell and US Lead Network, where he has revolutionized patient care and medical practice growth through innovative therapies and digital marketing strategies. He has authored two influential books on healthcare internet marketing, ranks among the top expert authors globally, and has been featured on the cover of Corporate Vision magazine for his impact on global regenerative therapies. Beyond his professional achievements, Dr. Greene is passionate about education, compassion, and continuous innovation.